1. Introduction - Why Tumor Marker Screening Matters
Cancer remains a major global health challenge. While tissue biopsy and imaging are gold standards, serum tumor marker testing provides a minimally invasive way to support early detection, disease monitoring, and recurrence surveillance, especially when combined in optimized diagnostic panels.
Among these markers, Carcinoembryonic Antigen (CEA) has been widely studied and used in clinical practice, especially for gastrointestinal malignancies.
2. CEA and Multi-Tumor Marker Diagnostics
What is CEA?
● Carcinoembryonic antigen (CEA) Test Kit is designed for the quantitative detection of CEA, a glycoprotein that is commonly elevated in gastrointestinal malignancies.
● Most clinically relevant in colorectal, gastric, and pancreatic cancers.
● Useful for early detection in high-risk populations and monitoring recurrence after treatment.
Combining CEA Testing with Other Relevant Markers
● Single CEA measurement may miss early-stage tumors.
● Multi-marker panels improve sensitivity and specificity by complementing CEA with other tumor-specific markers.
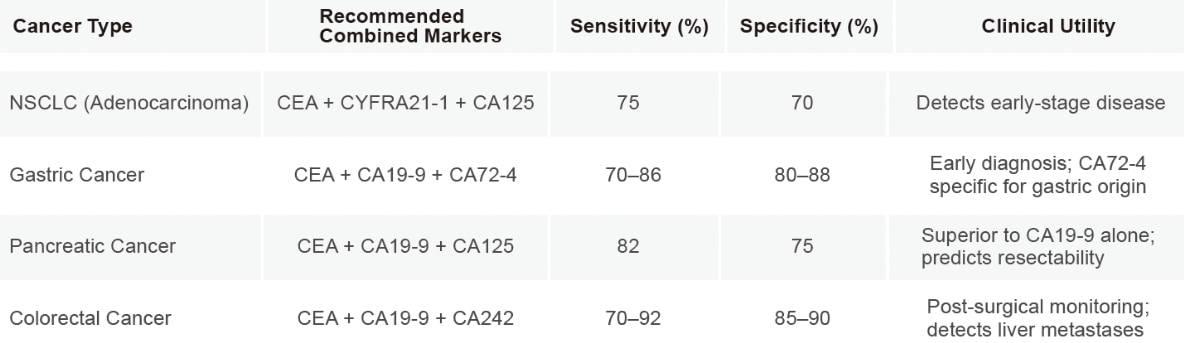

Key Takeaways:
Multi-marker panels improve early cancer detection beyond CEA alone.
Suitable for high-risk screening and post-treatment monitoring.
3. Poclight’s Innovative Tumor Marker Diagnostic Solutions
Poclight offers a comprehensive portfolio that empowers both distributors and laboratories to expand access to high-quality cancer diagnostics anywhere, anytime.
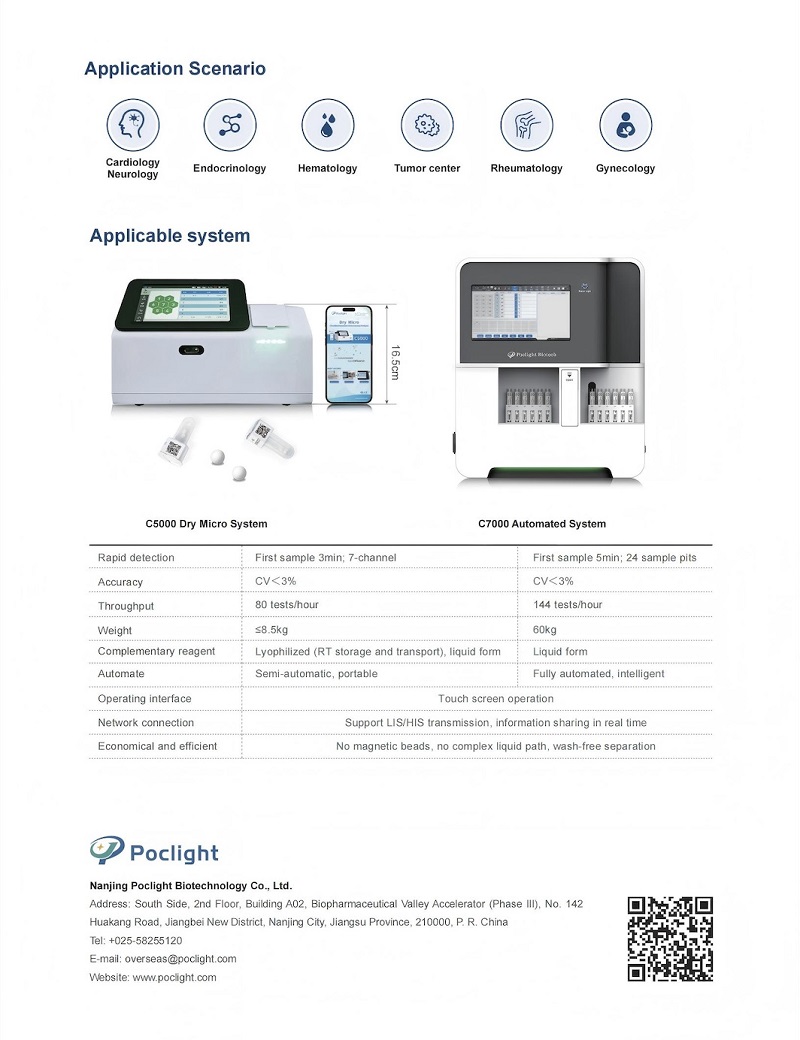
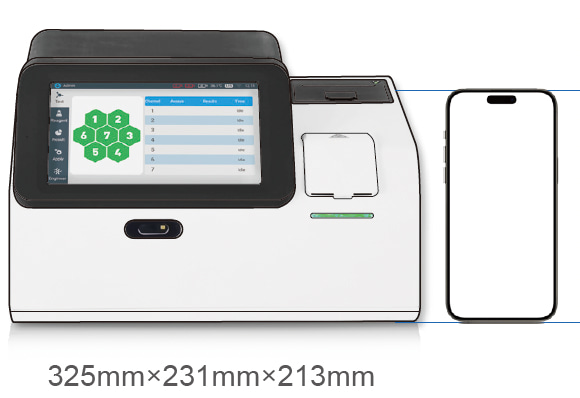
1) Advanced Platform: C5000 Dry Chemiluminescence Immunoassay Analyzer (Micro CLIA Analyzer)

2) Featured Tumor Marker Panel
✓ Complete tumor marker testing portfolio: PSA, CEA, AFP, CYFRA21-1, CA19-9, CA125
✓ Covers multiple major cancer types (liver, lung, prostate, gastrointestinal, ovarian)
✓ Fast, accurate, and suitable for hospitals, health centers, and primary care facilities
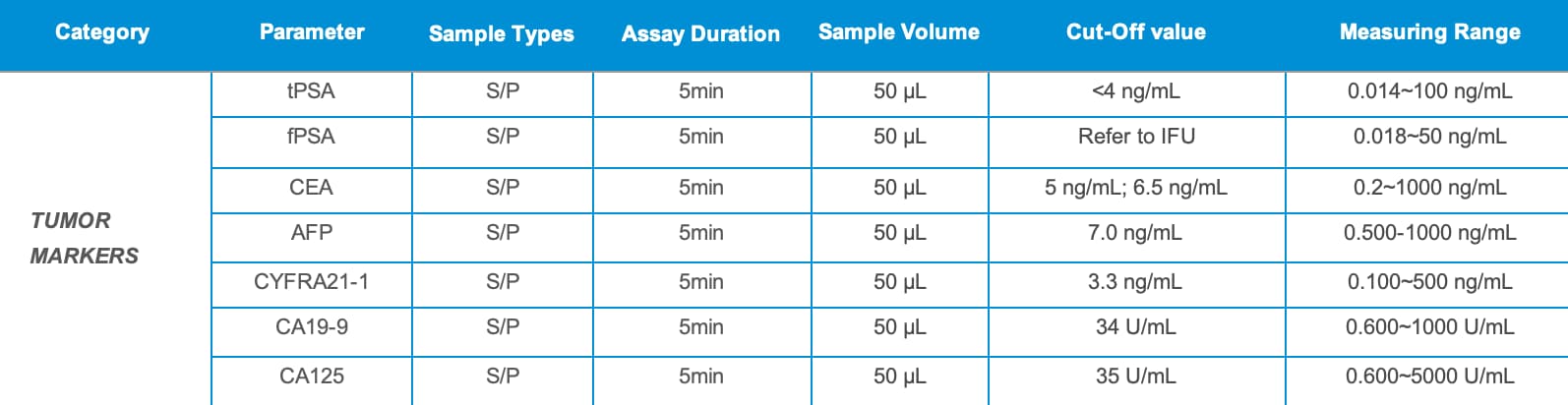
✓ Rapid detection in just 5 minutes, minimal sample volume of 50 µL, simple operation, low cost, high-quality CLIA methodology, innovative CRET patented technology, precise results, and a wide linear detection range.
✓ Ease of Use: Minimal training required

3) Cost & Efficiency Highlight
|
Feature |
Traditional CLIA Assay |
Poclight C5000 CLIA |
|
Turnaround Time |
15-30 min |
5 min |
|
Complexity |
High (trained technician required) |
Low (minimal training) |
|
Cost/ Case |
Expensive system $$$
50-100 tests/kit
lower per-test reagent cost for continuous high-volume processing |
Cost-efficient $
25 tests/kit
ideal for small labs & POCT |
Key Message: Poclight POC CLIA system reduces time, sample volume, and operational complexity, making multi-marker cancer screening more accessible and cost-effective.
More tumor marker and other assays in progress:PGⅠ|PGⅡ|HE4|CA15-3
Poclight Biotech is actively seeking global partners who share our vision for accessible, high-quality diagnostics. Interested in integrating CEA and other tumor marker diagnostics into your workflow or portfolio? Contact us to learn more.